A surgeon finishes a primary total knee arthroplasty at 7:45 AM. A femoral component, a tibial baseplate, a poly insert, a patellar button — all from your catalog. Your rep was in the room, standing next to the scrub tech through the entire case, tracking every box that got opened. They know exactly what was used.
It will take anywhere from 11 to 45 days, four people, and at least two phone calls before any of that information becomes an invoice — if it becomes an invoice at all.
This is the charge sheet problem. Not a technology problem. Not a training problem. A workflow problem that compounds every time your company adds a rep, a product line, or a hospital account — and the one that mid-level operations teams spend more time on than almost anything else they do.
What a Charge Sheet Actually Is
If you work in medical device operations, you already know. But it’s worth stating plainly, because the people making budget decisions sometimes don’t.
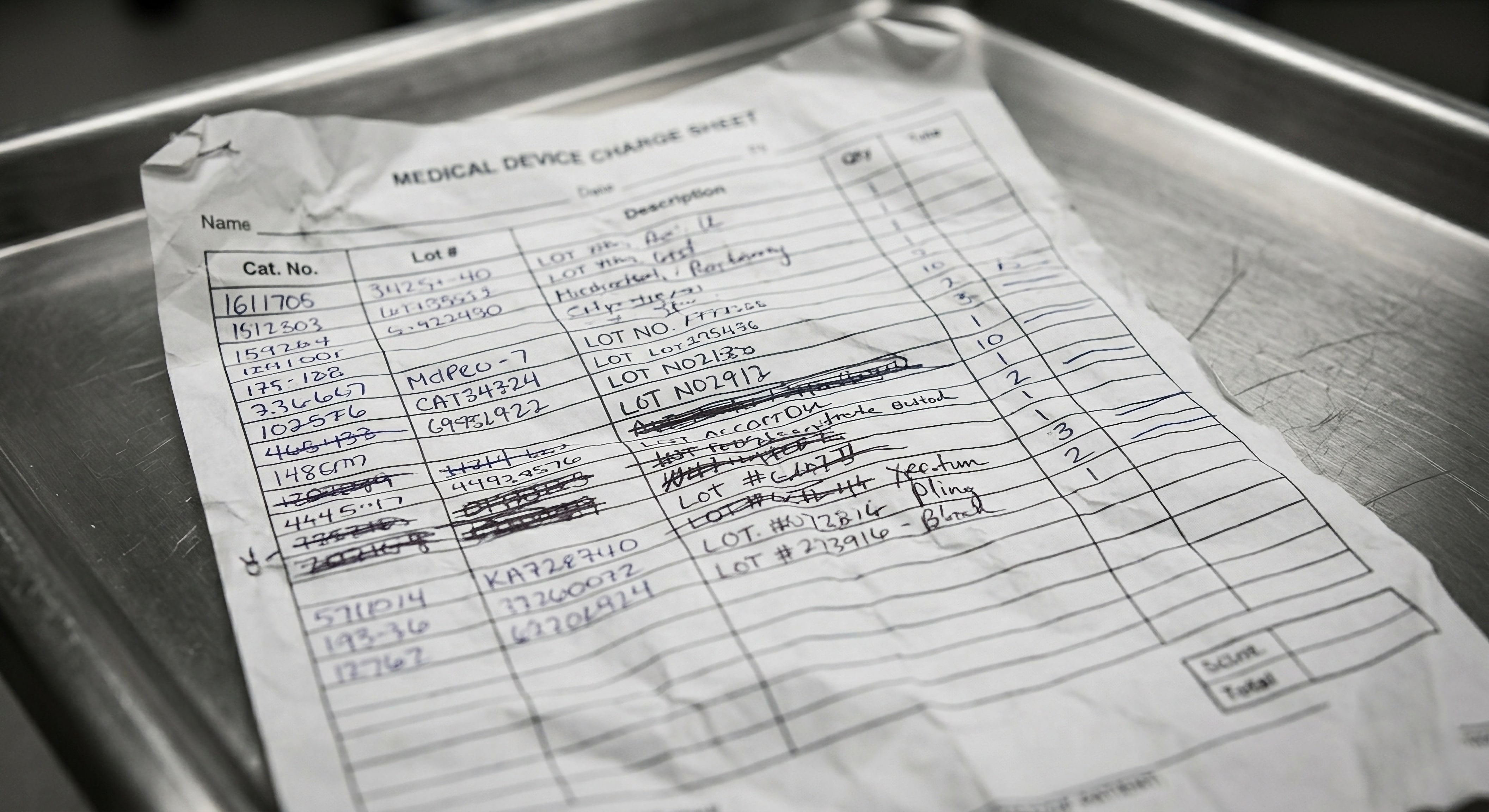
A charge sheet is the record of what was used during a surgical case. It captures more than most people outside of operations realize: which implants, which sizes, which catalog and lot numbers, which quantities — but also the facility where the procedure was performed, the surgeon, the date, and patient identifying information like name or medical record number. In some organizations it’s called a usage report, a case report, or an implant log. The name varies. What it documents doesn’t: what went into the patient, where, by whom, and what needs to be billed.
That patient information matters for two reasons. First, it’s how your team matches the charge sheet to the correct case when a hospital’s purchase order shows up days or weeks later. Second, it’s protected health information under HIPAA — which means the moment a rep photographs that form and texts it to a coordinator’s personal cell phone, you have PHI traveling through an unencrypted channel with no access controls and no audit trail. Every charge sheet that contains a patient name, MRN, or date of birth is a compliance event. Most mid-market manufacturers handle hundreds of these a month and don’t have a system in place that meets the HIPAA Security Rule’s transmission requirements.
In an ideal world, this record would be digital, standardized, encrypted in transit, and flow directly into your billing system. In the world most manufacturers actually operate in, it arrives as a photograph of a handwritten form — texted over iMessage or attached to a Gmail.
The Life of a Charge Sheet
Here’s what happens, step by step, between the OR and your ERP. If you manage this process, you’ll recognize every stage. If you oversee the team that manages it, this is what they’re doing instead of the work you keep asking them to prioritize.
Step 1: The rep fills it out.
After the case, the rep completes the charge sheet — usually on a paper form at the hospital, sometimes on the back of the rep case sheet they brought in. They’ve been tracking every box opened during the procedure, and now they need to transcribe the catalog numbers, lot numbers, quantities, implant sizes, the facility name, the surgeon, the procedure date, and some form of patient identification. That’s ten or more fields, most of them handwritten, while the room is being turned over for the next patient. The rep is writing complex alphanumeric lot numbers through a face mask, in a hurry, often with a next case to get to across town.
Some reps have clean handwriting and complete every field. Others — and this is a direct quote from a VP of Operations at a mid-size ortho manufacturer — produce forms where it looks like “somebody took a shotgun to it with ink.”
Step 2: The rep sends it.
The completed form gets photographed on a phone and texted or emailed to… someone. The coordinator. The CS inbox. The rep’s favorite person in the back office. There’s rarely a single, standardized channel for this. At one spinal implant manufacturer we talked to, reps were sending charge sheets to six different people depending on who they’d built a relationship with.
This is where the first delay happens. The rep is between cases. They’re driving. The photo sits in their camera roll for hours or days. When it does get sent, it arrives as a JPEG or PDF with no metadata, no case reference, and no indication of urgency.
Step 3: Someone reads it.
A member of your CS or operations team opens the photo and starts interpreting. This is skilled work — not because it requires special training, but because it requires pattern recognition that only comes from experience. They need to:
- Decipher the handwriting
- Identify which catalog numbers match your current product lines
- Verify that the lot numbers are real (not transposed, not from a recalled batch)
- Confirm the facility and match it to the correct account in the ERP
- Verify the surgeon against the facility’s records (because surgeons operate at multiple hospitals, and the billing terms differ by location)
- Determine which hospital and which purchasing agreement applies
- Figure out whether this is a consignment case, a bill-only, or a loaner return
And because the form contains patient information, the coordinator is now handling PHI — on a photo that arrived via text message, sitting in a shared inbox that five other people can access. The charge sheet needs to be processed and the patient data needs to be handled in compliance with HIPAA, but the workflow itself was never designed with that in mind.
If anything is unclear — and something is almost always unclear — they stop and go to Step 4.
Step 4: The investigation loop.
This is where the real time goes. The coordinator calls or texts the rep: “Can you confirm the lot number on the second implant? I can’t read it.” The rep is in surgery. No response for four hours. The coordinator moves on to other charge sheets. When the rep responds, the coordinator has moved to a different batch. The charge sheet goes back into the queue.
One operations director at a mid-size ortho manufacturer described it this way: “The order entry and transcribing isn’t too bad — it’s all the investigative work.” That tracks with what we see across the industry. The actual data entry — typing the information into the ERP — accounts for roughly 20% of the time spent processing a charge sheet. The other 80% is spent figuring out what the information actually is.
Missing lot numbers are the most common blocker. Unreadable handwriting is second. Pricing discrepancies — where the charge sheet says one thing and the contract says another — are third. Each blocker adds a cycle of back-and-forth that can stretch from hours to days.
Step 5: Data entry.
Once the coordinator has everything they need — confirmed quantities, verified catalog and lot numbers, matched pricing, correct PO reference — they type it into the ERP. NetSuite, SAP, Business Central, QAD, Macola, Epicor — the system varies, but the process is the same. Manual transcription from a photo to a structured database record.
This step is where the most common billing errors originate. A transposed catalog number. A pricing tier that doesn’t match the hospital’s contract. A lot number that’s one digit off. These aren’t careless mistakes — they’re the inevitable result of asking someone to manually transcribe data from a photograph of a handwritten form, hundreds of times a month, under time pressure.
Step 6: The PO that shows up three weeks later.
Here’s the part that makes this workflow fundamentally different from a normal data entry problem. In most industries, you get the purchase order first and then fulfill it. In medical devices — especially for bill-only and emergency cases — the surgery happens first. The PO arrives days or weeks later.
So your coordinator processes the charge sheet, enters the case data into the ERP, and then… waits. The hospital sends the PO when their procurement team gets around to it. When it arrives — sometimes a week later, sometimes a month — someone on your team has to match it back to the correct charge sheet. Which case was this for? Which surgeon, which date, which facility? If the PO references a different patient identifier than the charge sheet used, or lists the devices by a hospital-internal catalog number instead of yours, the matching becomes its own investigation.
This is where charge sheets go to die. The PO arrives, nobody can find the matching case without digging through emails and spreadsheets, and the whole thing goes into a “pending” pile that grows faster than anyone can work through it. The early-stage manufacturer who found “$60,000 sitting out there at hospitals” — that wasn’t charge sheets that never got submitted. It was charge sheets that got processed but never matched to a PO and invoiced. The work was done. The billing never happened.
Step 7: Invoice generation.
The ERP creates an invoice based on the entered data. If everything matches — the PO is on file, the pricing is correct, the quantities align — the invoice goes out. If anything doesn’t match, the invoice gets flagged and someone starts the investigation loop again, this time between your billing team and the hospital’s AP department.
Where the Money Disappears
The charge sheet workflow described above isn’t just slow. It’s where revenue goes to die.
The obvious cost is the labor: six CS reps at $60–80K each, all spending a significant portion of their day processing charge sheets that arrive as photographs. At one mid-size ortho manufacturer, the CS team manages a shared inbox where “everything starts,” with each person triaging, interpreting, investigating, and entering — and the CEO described the situation as “untenable.”
But the labor cost is the smaller problem. The larger one is the revenue that never gets captured at all.
Revenue disappears at two points. First, the submission gap: a charge sheet sits in a rep’s camera roll for a week, the case ages, and by the time anyone follows up, the details are fuzzy and the urgency is gone. Second — and this is the bigger one — the matching gap: the charge sheet was processed, the data was entered, but the PO arrived weeks later and nobody connected it back to the case. The surgery happened. The devices were used. The invoice never went out.
The Healthcare Financial Management Association estimates that poor charge capture processes cost hospitals 1–3% of net patient revenue annually. On the manufacturer side, the math is similar — and it compounds. Every charge sheet that falls out of the pipeline is a case that was completed, a device that was used, and revenue that was earned but never billed.
Why It Gets Worse as You Grow
The charge sheet problem has a particularly cruel scaling characteristic: the solutions that work at low volume actively break at higher volume.
At 50 cases a month, one experienced coordinator can hold the whole process in their head. They know which reps are reliable and which ones need reminders. They recognize the handwriting. They’ve memorized the top 30 catalog numbers. The spreadsheet they use to track pending charge sheets fits on one screen.
At 200 cases a month, that coordinator is underwater. The company hires a second, then a third. Now the institutional knowledge is fragmented — each person knows their reps but not the others’. The spreadsheet has too many tabs. Cases fall through because nobody is sure whose queue they’re in.
At 500 cases a month, you’re not adding incremental capacity. You’re “just burning cash,” as one ortho manufacturer CEO put it. Every new hire joins the same inbox, the same queue, the same manual process. You’re scaling the headcount but not the system.
This is the staircase-hiring problem. You don’t gradually need 10% more capacity — you suddenly can’t keep up, so you hire, then you have slack, then you suddenly can’t keep up again. Each new hire costs $60–80K but doesn’t change the underlying process. As one biologics manufacturer told us: “We’d rather spend that on a sales headcount than somebody in the back office. That’s the value proposition.”
The Lot Number Problem Within the Problem
Lot and serial number tracking deserves its own mention because it sits at the intersection of operational efficiency and regulatory compliance — and it’s the single most common field that’s missing or wrong on charge sheets.
FDA’s 21 CFR Part 821 requires manufacturers of certain implantable devices to maintain tracking records that can trace a device from manufacturing through distribution to the patient. When a charge sheet arrives with a missing or illegible lot number, your team isn’t just dealing with a billing delay. They’re dealing with a traceability gap that matters if there’s ever a recall.
The coordinator who can’t read the lot number has two options: chase the rep (delay), or guess based on what was supposed to be in the kit (risk). Neither option is good. Both happen every day.
This is the kind of operational detail that’s invisible to leadership until it becomes an audit finding. Mid-level operations staff carry this risk daily, for every charge sheet, and absorb the investigation time it takes to close the gap.
What Actually Has to Change
The temptation here is to prescribe a technology solution. And eventually, yes — the space between that handwritten form and your ERP is a gap that technology can close. But before reaching for a platform, there are structural problems worth addressing.
Standardize the input. The single biggest improvement most manufacturers can make is reducing the variability in how charge sheets arrive. This doesn’t require software. It requires a standard form (digital or paper), a single submission channel (email address, not six different coordinators’ cell phones), and a minimum set of required fields that the rep confirms before sending. Reps will comply if the path is easier than what they do today — and “email a photo to one address” is easier than “text whichever coordinator picks up.”
Separate transcription from investigation. Most operations teams handle both in the same pass: they read the charge sheet, find the gaps, chase the missing data, and enter the result. This means a single incomplete charge sheet blocks the coordinator from processing any others while they wait for a response. Splitting these into distinct steps — batch the transcription, batch the investigation, batch the entry — makes the bottleneck visible and measurable.
Measure what falls out. Almost no mid-market manufacturer tracks their charge sheet completion rate — the percentage of surgical cases where a charge sheet is submitted, processed, and invoiced within a target window. Without this metric, you can’t tell whether the problem is getting worse until a hospital account calls to complain or a quarterly audit reveals the gap. If you track one new number this quarter, make it this one.
The charge sheet is the starting point for everything downstream: the invoice, the revenue, the commission, the inventory adjustment, the compliance record. Every company in medical devices has this workflow. Very few have examined it closely enough to see where the time and money actually go.
The teams who process charge sheets know exactly where the problems are. They’ve been working around them for years. The question is whether the organization is ready to fix the workflow — or keep hiring people to absorb it.